



BANGKOK – A new approach to heart valve care is improving the lives for many patients in Thailand, particularly older individuals and those at high surgical risk, according to the Ministry of Public Health.
Transcatheter aortic valve implantation (TAVI) has been added under the ministry’s “Advanced & Smart: Accessible and Modern Medical Services” programme, said Dr Natthaphong Wongwiwat, director-general of the Department of Medical Services.
The Central Chest Institute of Thailand (CCIT) in Nonthaburi now utilizes TAVI to treat aortic valve stenosis, a condition in which the aortic valve narrows, blocking blood flow. The procedure eases symptoms, lowers complications, and supports quicker recovery, Dr Natthaphong said.
Aortic valve stenosis can develop with age or be present from birth, such as in patients with a bicuspid aortic valve. Over time, calcium can build up on the valve, causing stiffness and poor opening, which increases strain on the heart.
Dr Anek Kanoksilp, director of the CCIT, said TAVI is a safe and effective option for people who cannot have open-heart surgery, especially those over 80 years old or living with several chronic illnesses.
This minimally invasive technique places a new valve via a catheter guided through a blood vessel in the groin, so patients avoid major surgery. Recovery is faster, risks are reduced, and quality of life improves.
The CCIT first carried out TAVI in 2015 under a royal project honouring the 60th birthday of Her Royal Highness Princess Maha Chakri Sirindhorn. The programme began with 10 patients and has grown since then.
A TAVI Training Centre opened in 2021 to build skills across Thailand and Asean. More than 120 patients have been treated to date.
 Aorta Heart Valve
Aorta Heart Valve
Stroke care expansion using mechanical thrombectomy
The Department of Medical Services plans to widen access to mechanical thrombectomy, an endovascular treatment for acute ischaemic stroke.
The goal is to set up a mechanical thrombectomy centre in every health region, in line with the ministry’s focus on restoring quality of life and reducing disability after stroke, said Dr Natthaphong.
The Neurological Institute of Thailand in Bangkok has offered endovascular thrombectomy (EVT) since June 2015. It has treated more than 1,100 patients using this catheter-based method.
The institute has also transferred the know-how to regional hospitals nationwide, with the target of a mechanical thrombectomy centre in each health region, Dr Natthaphong added.
The rollout is backed by a policy that provides full reimbursement under the Universal Coverage for Emergency Patients (UCEP) scheme when referrals are needed because a hospital’s capacity is exceeded.
Dr Tassanee Tantiritsak, acting director of the institute, said EVT achieves a successful clot removal rate of 80 to 90 percent with a low rate of side effects and complications. The rate of intracerebral hemorrhage after the procedure is 4.2 percent.
According to Dr Tassanee, outcomes show high procedural success, strong clinical results, and a solid safety profile, with clear reductions in disability and death among stroke patients.
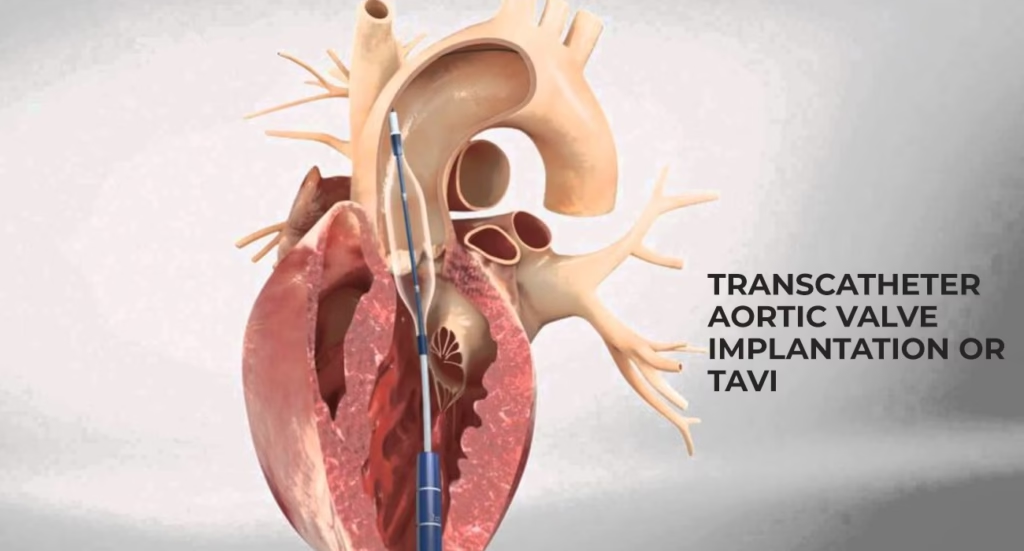
Transcatheter aortic valve implantation (TAVI)
Transcatheter Aortic Valve Implantation (TAVI), also called Transcatheter Aortic Valve Replacement (TAVR), is a minimally invasive treatment for severe aortic stenosis. It is often used for people at high or intermediate risk from open-heart surgery, and is now considered for selected low-risk patients.
What is aortic stenosis?
- The aortic valve becomes narrowed, which limits blood flow from the left ventricle to the aorta.
- Most often seen in older adults due to calcium build-up.
- Common symptoms include chest pain, breathlessness, fainting, and signs of heart failure.
How TAVI works
- Valve types
- Balloon-expandable valves, for example, the Edwards SAPIEN range
- Self-expanding valves, for example, Medtronic CoreValve or Evolut, and Boston Scientific Lotus
- Access routes, in preferred order
- Transfemoral, via the groin artery, is used in about 90% of cases
- Transapical, through a small incision to the left ventricle
- Transaortic, through the ascending aorta
- Subclavian or axillary, carotid, or caval-aortic routes as alternatives
- Key steps
- Performed with general anesthesia or conscious sedation
- A catheter carries a compressed valve through the chosen vessel
- The new valve is positioned inside the diseased native valve
- Deployment with balloon inflation or self-expansion
- The original valve leaflets are pressed against the aortic wall
Indications (ACC/AHA 2020 guidance)
| Risk category | Recommendation |
|---|---|
| High surgical risk | TAVI is preferred over SAVR |
| Intermediate risk | TAVI is a reasonable alternative to SAVR |
| Low risk (over 75 years, or younger with favourable anatomy) | TAVI has been approved by the FDA since 2019 |
Contraindications
- Bicuspid aortic valve with poor anatomical suitability
- Severe aortic regurgitation
- Active infective endocarditis
- Life expectancy under 1 year
- Vessels too small or diseased for safe access
Complications
| Complication | Incidence |
|---|---|
| Stroke | 2 to 5% |
| Vascular complications | 5 to 10% |
| Need for a permanent pacemaker | 10 to 25% (higher with self-expanding valves) |
| Paravalvular leak | 5 to 40% mild, under 1% severe |
| Acute kidney injury | 5 to 15% |
| 30-day mortality | 1 to 3% in low-risk, 3 to 6% in high-risk |
Care after the procedure
- Dual antiplatelet therapy with aspirin plus clopidogrel for 1 to 6 months
- Long-term aspirin after that
- Echocardiogram before discharge
- Follow-up at 1 month, 1 year, then once a year
Outcomes from major trials
| Trial | Population | Main outcome |
|---|---|---|
| PARTNER 1 (2011) | Inoperable | TAVI is better than medical therapy |
| CoreValve US Pivotal (2014) | High risk | TAVI is better than SAVR for survival |
| PARTNER 2 (2016) | Intermediate risk | TAVI is comparable to SAVR |
| PARTNER 3 (2019) | Low risk | TAVI is superior to SAVR for death, stroke, and rehospitalization |
| Evolut Low Risk (2019) | Low risk | TAVI non-inferior to SAVR |
What is next
- Valve-in-valve TAVI for failing surgical bioprosthetic valves
- Studying TAVI for moderate aortic stenosis with heart failure, for example, TAVR UNLOAD and PROGRESS
- Cerebral embolic protection devices, such as Sentinel CPS
- Next-generation valves with slimmer profiles, repositioning features, and lower paravalvular leak rates
Summary
TAVI has transformed the management of aortic stenosis for suitable patients across risk groups. Recovery is often quicker than with surgical aortic valve replacement, with typical hospital stays of 1 to 3 days compared with 5 to 7 days for surgery. Decisions should be made by a multidisciplinary Heart Team.









